Chronic stable angina: treatment options
BMJ 2003; 326 doi: https://doi.org/10.1136/bmj.326.7400.1185 (Published 29 May 2003) Cite this as: BMJ 2003;326:1185
- Laurence O'Toole, consultant cardiologist and physician,
- Ever D Grech, consultant cardiologist, assistant professor
- Royal Hallamshire Hospital, Sheffield, Health Sciences Centre and St Boniface Hospital, Winnipeg, Manitoba, Canada, University of Manitoba, Winnipeg
Introduction
In patients with chronic stable angina, the factors influencing the choice of coronary revascularisation therapy (percutaneous coronary intervention or coronary artery bypass surgery) are varied and complex. The severity of symptoms, lifestyle, extent of objective ischaemia, and underlying risks must be weighed against the benefits of revascularisation and the patient's preference, as well as local availability and expertise. Evidence from randomised trials and large revascularisation registers can guide these decisions, but the past decade has seen rapid change in medical treatment, bypass surgery, and percutaneous intervention. Therefore, thought must be given to whether older data still apply to contemporary practice.
Major factors influencing risks and benefits of coronary revascularisation

Top: Diagrams of saphenous vein and left internal mammary artery grafts for coronary artery bypass surgery. Bottom: Three completed grafts—(1) left internal mammary artery (LIMA) to left anterior descending artery (LAD), and saphenous vein grafts (SVG) to (2) diagonal artery (DG) and (3) obtuse marginal artery (OM)
{kind=link}

Top: Diagrams of saphenous vein and left internal mammary artery grafts for coronary artery bypass surgery. Bottom: Three completed grafts—(1) left internal mammary artery (LIMA) to left anterior descending artery (LAD), and saphenous vein grafts (SVG) to (2) diagonal artery (DG) and (3) obtuse marginal artery (OM)
{kind=link}
Patients with chronic stable angina have an average annual mortality of 2-3%, only twice that of age matched controls, and this relatively benign prognosis is an important consideration when determining the merits of revascularisation treatment. Certain patients, however, are at much higher risk. Predictors include poor exercise capacity with easily inducible ischaemia or a poor haemodynamic response to exercise, angina of recent onset, previous myocardial infarction, impaired left ventricular function, and the number of coronary vessels with significant stenoses, especially when disease affects the left main stem or proximal left anterior descending artery. Although the potential benefits of revascularisation must be weighed against adverse factors, those most at risk may have the most to gain.
Treatment strategies
Medical treatment
Anti-ischaemic drugs improve symptoms and quality of life, but have not been shown to reduce mortality or myocardial infarction. βblockers may improve survival in hypertension, in heart failure, and after myocardial infarction, and so are considered by many to be first line treatment. Nicorandil has recently been shown to reduce ischaemic events and need for hospital admission.
Risk score for assessing probable mortality from bypass surgery in patients with chronic sTable angina
Trials comparing medical treatment with revascularisation predate the widespread use of antiplatelet and cholesterol lowering drugs. These drugs reduce risk, both in patients treated with drugs only and in those undergoing revascularisation, and so may have altered the risk-benefit ratio for a particular revascularisation strategy in some patients.
Coronary artery bypass graft surgery
Coronary artery bypass surgery involves the placement of grafts to bypass stenosed native coronary arteries, while maintaining cerebral and peripheral circulation by cardiopulmonary bypass. The grafts are usually saphenous veins or arteries (principally the left internal mammary artery).
Operative mortality is generally 1-3% but may be much higher in certain subsets of patients. Scoring systems can predict operative mortality based on clinical, investigational, and operative factors. Important developments that have occurred since trials of bypass surgery versus medical treatment were conducted include increased use of arterial grafts (which have much greater longevity than venous grafts), surgery without extracorporeal circulation (“off-pump” bypass), and minimal access surgery.
Percutaneous coronary intervention
The main advantages of percutaneous intervention over bypass surgery are the avoidance of the risks of general anaesthesia, uncomfortable sternotomy and saphenous wounds, and complications of major surgery (infections and pulmonary emboli). Only an overnight hospital stay is necessary (and many procedures can be performed as day cases), and the procedure can be easily repeated. The mortality is low (0.2%), and the most serious late complication is restenosis.
Patient suitability is primarily determined by technical factors. A focal stenosis on a straight artery without proximal vessel tortuousness or involvement of major side branches is ideal for percutaneous intervention. Long, heavily calcified stenoses in tortuous vessels or at bifurcations and chronic total occlusions are less suitable. This must be borne in mind when interpreting data from trials of percutaneous intervention and bypass surgery, as only a minority of patients were suitable for both procedures. Nowadays, more and more patients undergo percutaneous intervention, and referral rates for bypass surgery are falling.
Subgroup analysis of mortality benefit from coronary artery bypass surgery compared with medical treatment at 10 years after randomisation for patients with chronic stable angina
Comparative studies of revascularisation strategies
Coronary artery bypass surgery versus medical treatment
In a meta-analysis of seven trials comparing bypass surgery with medical treatment, surgery conferred a survival advantage in patients with severe left main stem coronary disease, three vessel disease, or two vessel disease with severely affected proximal left anterior descending artery. The survival gain was more pronounced in patients with left ventricular dysfunction or a strongly positive exercise test. However, only 10% of trial patients received an internal mammary artery graft, only 25% received antiplatelet drugs, and the benefit of lipid lowering drugs on long term graft patency was not appreciated when these studies were carried out. Furthermore, 40% of the medically treated patients underwent bypass surgery during 10 years of follow up. Thus, these data may underestimate the benefits of surgery compared with medical treatment alone.

Left: Angiogram of a 10 year old diseased venous graft to the obtuse marginal artery showing proximal aneurysmal dilatation (A) and severe stenosis in middle segment (B). Right: Removal of this graft after repeat bypass surgery shows its gross appearance (graft longitudinally opened in right image), with atherosclerosis in a thin walled aneurysm and a small residual lumen
{kind=link}

Left: Angiogram of a 10 year old diseased venous graft to the obtuse marginal artery showing proximal aneurysmal dilatation (A) and severe stenosis in middle segment (B). Right: Removal of this graft after repeat bypass surgery shows its gross appearance (graft longitudinally opened in right image), with atherosclerosis in a thin walled aneurysm and a small residual lumen
{kind=link}

Left: Angiogram of a 10 year old diseased venous graft to the obtuse marginal artery showing proximal aneurysmal dilatation (A) and severe stenosis in middle segment (B). Right: Removal of this graft after repeat bypass surgery shows its gross appearance (graft longitudinally opened in right image), with atherosclerosis in a thin walled aneurysm and a small residual lumen
{kind=link}
In lower risk patients bypass surgery is indicated only for symptom relief and to improve quality of life when medical treatment has failed. Surgery does this effectively, with 95% of patients gaining immediate relief from angina and 75% remaining free from angina after five years. Unfortunately, venous grafts have a median life span of only seven years, and after 15 years only 15% of patients are free from recurrent angina or death or myocardial infarction. However, the increased use of internal mammary artery grafts, which have excellent long term patency (85% at 10 years), has increased postoperative survival and reduced long term symptoms.

Old saphenous vein grafts may contain large amounts of necrotic clotted debris, friable laminated thrombus, and ulcerated atheromatous plaque and are unattractive for percutaneous intervention because of the high risk of distal embolisation. However, distal embolisation protection devices such as the FilterWire EX (far right) reduce this risk by trapping any material released. Such a device (far left, B) is positioned in the distal segment of a subtotally occluded saphenous vein graft of the left anterior descending artery (A) before it is dilated and stented (inner left, C) to restore blood flow (inner right)
{kind=link}

Old saphenous vein grafts may contain large amounts of necrotic clotted debris, friable laminated thrombus, and ulcerated atheromatous plaque and are unattractive for percutaneous intervention because of the high risk of distal embolisation. However, distal embolisation protection devices such as the FilterWire EX (far right) reduce this risk by trapping any material released. Such a device (far left, B) is positioned in the distal segment of a subtotally occluded saphenous vein graft of the left anterior descending artery (A) before it is dilated and stented (inner left, C) to restore blood flow (inner right)
{kind=link}

Old saphenous vein grafts may contain large amounts of necrotic clotted debris, friable laminated thrombus, and ulcerated atheromatous plaque and are unattractive for percutaneous intervention because of the high risk of distal embolisation. However, distal embolisation protection devices such as the FilterWire EX (far right) reduce this risk by trapping any material released. Such a device (far left, B) is positioned in the distal segment of a subtotally occluded saphenous vein graft of the left anterior descending artery (A) before it is dilated and stented (inner left, C) to restore blood flow (inner right)
{kind=link}

Old saphenous vein grafts may contain large amounts of necrotic clotted debris, friable laminated thrombus, and ulcerated atheromatous plaque and are unattractive for percutaneous intervention because of the high risk of distal embolisation. However, distal embolisation protection devices such as the FilterWire EX (far right) reduce this risk by trapping any material released. Such a device (far left, B) is positioned in the distal segment of a subtotally occluded saphenous vein graft of the left anterior descending artery (A) before it is dilated and stented (inner left, C) to restore blood flow (inner right)
{kind=link}
Percutaneous coronary intervention versus medical treatment
Most percutaneous procedures are undertaken to treat single vessel or two vessel disease, but few randomised controlled trials have compared percutaneous intervention with medical treatment. These showed that patients undergoing the percutaneous procedure derived greater angina relief and took less drugs but required more subsequent procedures and had more complications (including non-fatal myocardial infarction), with no mortality difference. Patients with few symptoms did not derive benefit. Therefore, percutaneous intervention is suitable for low risk patients with one or two vessel disease and poor symptom control with drugs, at a cost of a slightly higher risk of non-fatal myocardial infarction. However, the procedure may not be indicated if symptoms are well controlled.

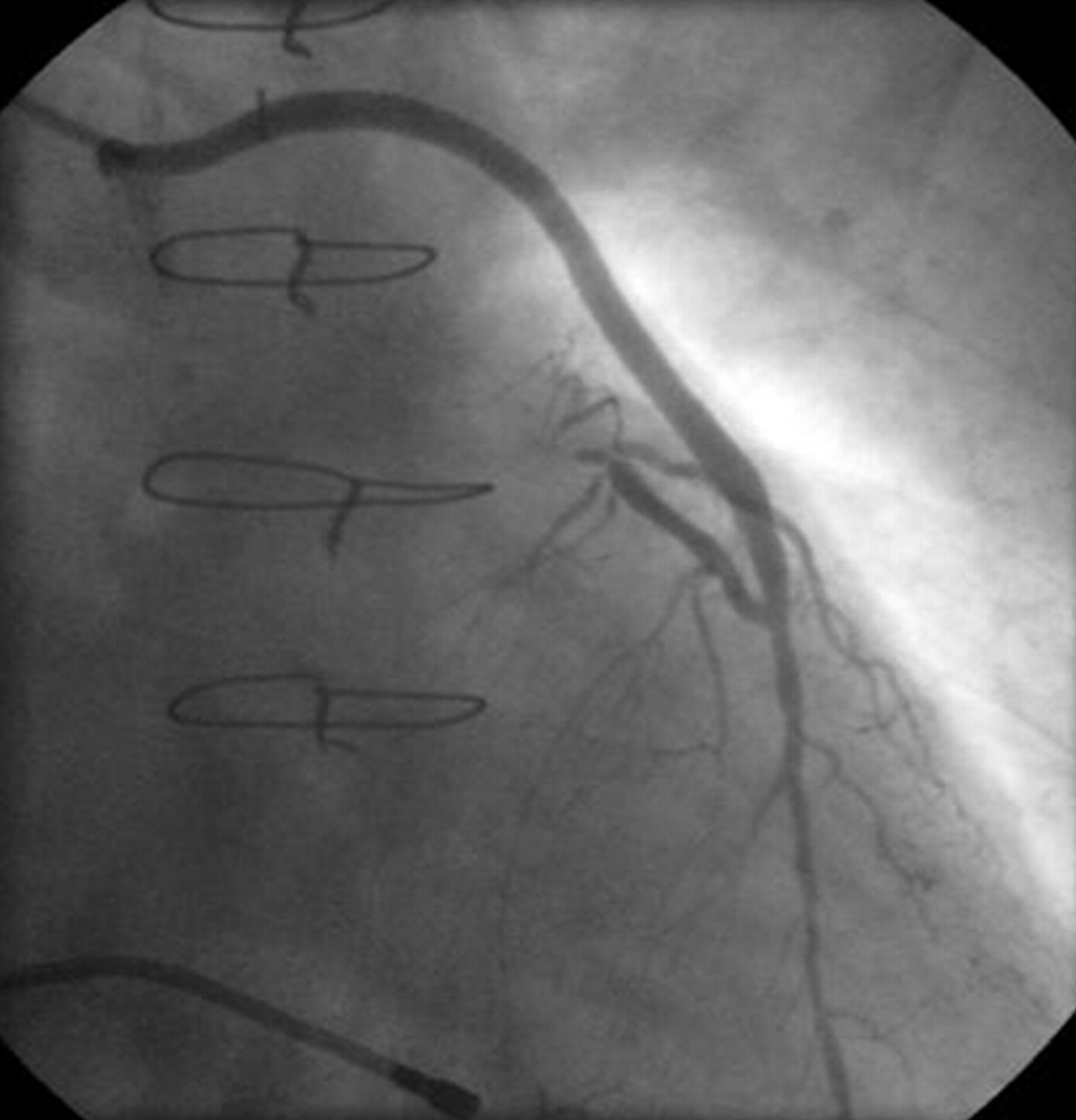
Coronary angiogram showing a severe focal stenosis (arrow) in a large oblique marginal branch of the left circumflex artery (LCx), suitable for percutaneous coronary intervention. The left anterior descending artery (LAD) has no important disease
{kind=link}
Percutaneous intervention versus bypass surgery
Single vessel disease
In a meta-analysis by Pocock et al percutaneous intervention in patients with single vessel disease resulted in mortality similar to that found with bypass surgery (3.7% v 3.1% respectively) but a higher rate of non-fatal myocardial infarction (10.1% v 6.1%, P=0.04). Angina was well treated in both groups, but persistence of symptoms was slightly higher with percutaneous intervention. Rates of repeat revascularisation were much higher with percutaneous intervention than bypass surgery.

Coronary angiograms of 70 year old woman with limiting angina. There were severe stenoses (arrows) in the proximal and middle left anterior descending artery (LAD, top) and in the distal right coronary artery (RCA, left). Because of the focal nature of these lesions, percutaneous coronary intervention was the preferred option
{kind=link}

Coronary angiograms of 70 year old woman with limiting angina. There were severe stenoses (arrows) in the proximal and middle left anterior descending artery (LAD, top) and in the distal right coronary artery (RCA, left). Because of the focal nature of these lesions, percutaneous coronary intervention was the preferred option
{kind=link}
Multivessel disease
Since comparative trials could recruit only those patients who were suitable for either revascularisation strategy, only 3-7% of screened patients were included. These were predominantly “low risk” patients with two vessel disease and preserved left ventricular function—patients in whom bypass surgery has not been shown to improve survival—and thus it is unlikely that a positive effect in favour of percutaneous intervention would have been detected. The generally benign prognosis of chronic stable angina means that much larger trials would have been required to show significant differences in mortality.
A meta-analysis of data available to the end of 2000 revealed similar rates of death and myocardial infarction with both procedures, but repeat revascularisation rates were higher with percutaneous intervention. The prevalence of appreciable angina was greater with percutaneous intervention at one year, but this difference disappeared at three years.

Coronary angiograms of a 69 year old man with limiting angina and exertional breathlessness. There was severe proximal disease (arrows) of the left anterior descending (LAD) and left circumflex arteries (LCx) (top) and occlusion of the right coronary artery (RCA, left). The patient was referred for coronary artery bypass surgery on prognostic and symptomatic grounds
{kind=link}

Coronary angiograms of a 69 year old man with limiting angina and exertional breathlessness. There was severe proximal disease (arrows) of the left anterior descending (LAD) and left circumflex arteries (LCx) (top) and occlusion of the right coronary artery (RCA, left). The patient was referred for coronary artery bypass surgery on prognostic and symptomatic grounds
{kind=link}
The nature of percutaneous coronary intervention has changed considerably over the past 10 years, with important developments including stenting and improved antiplatelet drugs. The integrated use of these treatments clearly improves outcomes, but almost all of the revascularisation trials predate these developments.
A more recent trial comparing percutaneous intervention and stenting with bypass surgery in multivessel disease confirmed similar rates of death, myocardial infarction, and stroke at one year, with much lower rates of repeat revascularisation after percutaneous intervention compared with earlier trials. There was also a cost benefit of nearly $3000 (£1875) per patient associated with percutaneous intervention at 12 months. The recent introduction of drug eluting (coated) stents, which seem to reduce substantially the problem of restenosis, is likely to extend the use of percutaneous intervention in multivessel disease over the next few years.
Diabetes
Bypass surgery confers a survival advantage in symptomatic diabetic patients with multivessel disease The BARI trial revealed a significant difference in five year mortality (21% with percutaneous intervention v 6% with bypass surgery). Similar trends have been found in other large trials. However, the recent RAVEL and SIRIUS studies, in which the sirolimus eluting Cypher stent was compared with the same stent uncoated, showed a remarkable reduction in restenosis rates within the stented segments in diabetic patients (0% v 42% and 18% v 51% respectively). Ongoing trials will investigate this issue further.
Names of trials
Other study data
Large registries of outcomes in patients undergoing revascularisation have the advantage of including all patients rather than the highly selected groups included in randomised trials. The registry data seem to agree with those from randomised trials: patients with more extensive disease fare better with bypass surgery, whereas percutaneous intervention is preferable in focal coronary artery disease.
Emerging treatment options for refractory angina
An unusual observation is that patients screened and considered suitable for inclusion in a trial fared slightly better if they refused to participate than did those who enrolled. The heterogeneous nature of coronary disease means that certain patient subsets will probably benefit more from one treatment than another. The better outcome in the patients who were suitable but not randomised may indicate that cardiologists and surgeons recognise which patients will benefit more from a particular strategy—subtleties that are lost in the randomisation process of controlled trials.
Refractory coronary artery disease
Increasing numbers of patients with coronary artery disease have angina that is unresponsive to both maximal drug treatment and revascularisation techniques. Many will have already undergone multiple percutaneous interventions or bypass surgery procedures, or have diffuse and distal coronary artery disease. In addition to functional limitations, their prognosis may be poor because of impaired ventricular function. Emerging treatments may provide alternative symptomatic improvement for some patients. There is also renewed interest in the potential anti-ischaemic effects of angiotensin converting enzyme inhibitors and the plaque stabilising properties of statins.
Further reading
Footnotes
-
The ABC of interventional cardiology is edited by Ever D Grech and will be published as a book in summer 2003.
The picture showing three completed coronary artery bypass grafts and the pictures of a 10 year old diseased venous graft to the obtuse marginal artery were provided by G Singh, consultant cardiothoracic surgeon, Heath Sciences Centre, Winnipeg, E Pascoe, consultant cardiothoracic surgeon, St Boniface Hospital, Winnipeg, and J Scatliff, consultant anaesthetist, St Boniface Hospital. The picture of the FilterWire EX distal embolisation protection device was provided by Boston Scientific Corporation, Minneapolis, USA.
-
Competing interests None declared.