Anticipating and managing postoperative delirium and cognitive decline in adults
BMJ 2011; 343 doi: https://doi.org/10.1136/bmj.d4331 (Published 20 July 2011) Cite this as: BMJ 2011;343:d4331
- Robert D Sanders, Medical Research Council clinical training fellow12,
- Pratik P Pandharipande, associate professor34,
- Andrew J Davidson, associate professor56,
- Daqing Ma, senior lecturer1,
- Mervyn Maze, professor7
- 1Magill Department of Anaesthetics, Intensive Care, and Pain Medicine, Imperial College London, Chelsea and Westminster Hospital, London SW10 9NH, UK
- 2Department of Leucocyte Biology, Imperial College London
- 3Anesthesiology Service, VA TN Valley Health Care System, Nashville, TN, USA
- 4Department of Anesthesiology, Division of Critical Care, Vanderbilt University School of Medicine, Nashville
- 5Department of Anaesthesia, Royal Children’s Hospital, Melbourne, Australia
- 6Anaesthesia Research Group, Murdoch Children’s Research Institute, Melbourne
- 7Department of Anesthesia and Perioperative Care, University of California, San Francisco, CA 94143-0648, USA
- Correspondence to: R D Sanders robert.sanders{at}imperial.ac.uk
- Accepted 4 July 2011
The brain is vulnerable during the perioperative period in people of all ages. Neurobehavioural disturbances are common complications of perioperative care, manifesting in three distinct forms: emergence delirium, postoperative delirium, and postoperative cognitive decline. Delirium is defined by the presence of disturbed consciousness (reduced clarity of awareness of the environment with reduced ability to focus, sustain, or shift attention) and a change in cognition (such as memory deficit, disorientation, or language disturbance) or the development of a perceptual disturbance that is not better accounted for by a pre-existing, established, or evolving dementia. Emergence delirium occurs on emergence from anaesthesia and sedation, with no lucid interval, and lasts approximately 30 minutes. Postoperative delirium lasts hours or longer, with or without lucid intervals. Postoperative cognitive decline refers to a more subtle cognitive impairment noted on neuropsychological tests that typically assess attention and memory.
Postoperative delirium is the most severe of the three disorders, tantamount to an acute brain failure, and should be considered akin to other postoperative organ failures. We review delirium and long term cognitive decline associated with perioperative care in adults and discuss potential mechanisms and preventive/intervention strategies in light of recent randomised controlled trials, meta-analyses, and prospective cohort studies.
Sources and selection criteria
Each author had previously conducted a search of published work. In addition a formal Medline search was undertaken in March 2011 with keywords “delirium”, “hip”, and “fracture” to provide data for the figure. Studies were identified by RDS and selected based on published criteria for meta-analysis10 by Nina Frasen. Joost Witlox and Pim Van Gool analysed the data and kindly provided the figure.
Who is at risk of postoperative neurobehavioural disturbance?
Young adults seem particularly vulnerable to emergence delirium, whereas in older patients (over 60) postoperative delirium, and its subsequent sequelae, are more common. Three large cohort studies have shown that emergence delirium occurs in about 5-21% of adults (diagnosed using the agitation components of sedation scales).1 2 3 Emergence delirium typically affects young, healthy, often male adults who have preoperative anxiety, those who are given benzodiazepine premedication, and those who undergo lengthy invasive surgery. Preoperative benzodiazepine seems to be the strongest risk factor (odds ratio [OR] 1.9, 95% confidence interval 1.1 to 3.3).1
Based primarily on cohort studies, the more prolonged postoperative delirium affects 14-24% of adult hospital admissions, 3-53% of postoperative patients undergoing major surgery, and as many as 83% of critically ill patients.4 5 Systematic reviews have shown a particularly high incidence of delirium in elective orthopaedic surgery (3-27%) and surgery after hip fracture (4-53%).5 Reported rates of 29-39% after vascular surgery and 3-47% after cardiac surgery indicate that delirium is a prevalent complication of major surgery. Variation in reported incidence probably reflects differences in methods of diagnosing delirium and varied severity of surgery. Modifiable and non-modifiable risk factors for postoperative delirium are presented in box 1.
Box 1 Risk factors for postoperative delirium
Non-modifiable
Age
Cognitive impairment
Dementia
Depression
Comorbid diseases (such as renal failure)
Type/severity of surgery
Genetic factors (such as sigma 4 allele of apolipoprotein E4)
Modifiable
Infection and inflammation
Metabolite disturbances
Medication
Pain and discomfort (for example, from a urinary catheter)
Sleep disruption
What causes postoperative delirium?
Various theories have been advanced about the pathogenesis of delirium, but none adequately accounts for the diverse risk factors and heterogeneity in presentation of the syndrome. Deranged neurotransmission (for example, gamma-amino-butyric acid, dopamine, or acetylcholine signalling), perhaps provoking altered network connectivity in the brain, has been suggested as a possible cause.4 6 Additionally, neuroinflammation, and in particular microglial activation, is increasingly recognised as a pivotal factor in the disruption of cognition postoperatively.7 8
How is postoperative delirium diagnosed?
Postoperative delirium may occur after a lucid interval and can last days or weeks. Delirium may take a hypoactive form (symptoms such as inattention and lethargy), a hyperactive form (aggressive behaviour, pulling catheters, and so on), or a mixture of these forms. Signs include fluctuating levels of consciousness, inattention, disorganised thinking, and perceptual disturbances such as hallucinations and delusions. In box 2 we present the confusion assessment method scale for the diagnosis of delirium in adults,9 which has a sensitivity of 94% and a specificity of 89%. Because the hypoactive form of delirium can be particularly difficult to detect, validated methods to diagnose delirium are in demand. A missed diagnosis of delirium has been associated with increased mortality,4 yet delirium is not routinely assessed in the postoperative period.
Box 2 Confusion assessment method scale for diagnosis of delirium in adults9
The diagnosis of delirium requires a present or abnormal rating for criteria 1 and 2 plus either 3 or 4.
1) Acute onset and fluctuating course: Is there evidence of an acute change in mental status from the patient’s baseline? Did the patient’s behaviour fluctuate during the day—did it come and go or increase and decrease in severity? (Information from a family member or carers may be needed)
2) Inattention: Does the patient have difficulty focusing attention—are they easily distracted or do they have difficulty keeping track of what is being said? (Inattention can be detected by the digit span test or by asking for the days of the week to be recited backwards)
3) Disorganised thinking: Is the patient’s speech disorganised or incoherent, or is there an unclear or illogical flow of ideas, or unpredictable switching between subjects?
4) Altered level of arousal: Overall, would you rate this patient’s level of arousal as alert (normal), vigilant (hyperalert), lethargic (drowsy, easily aroused), stupor (difficult to rouse), or coma (cannot be roused)? All ratings except alert are scored as abnormal.
What are the possible consequences of postoperative delirium?
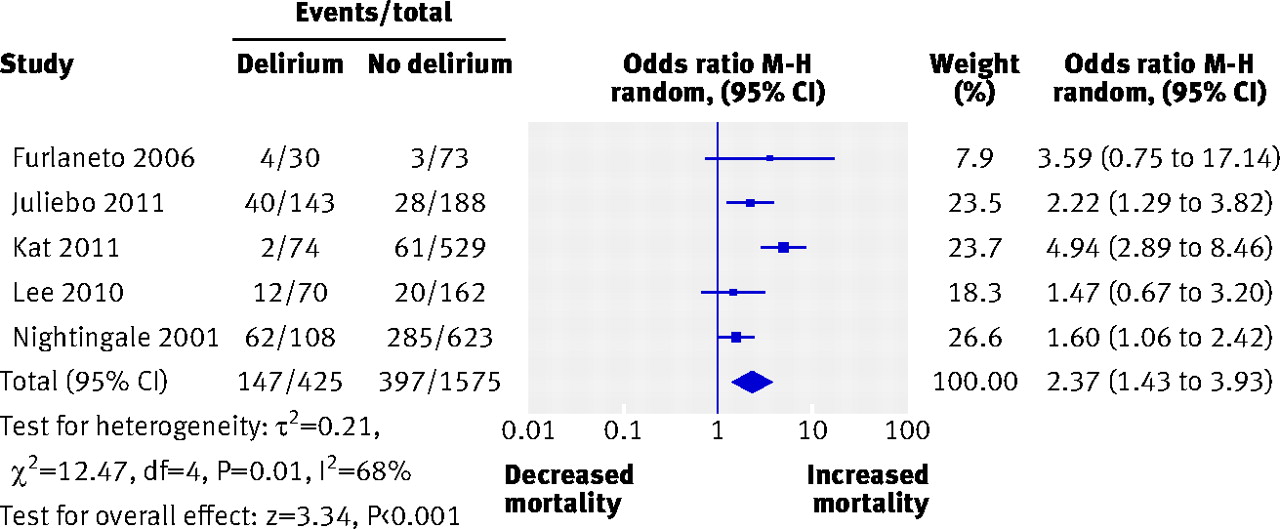
A recent meta-analysis showed a doubling of the hazard ratio for death after an episode of delirium in a mixture of medical and surgical patients (OR 1.95, 95% confidence interval 1.51-2.52) over an average 22.7 month follow-up period.10 Associated increases in the risk of admission to an institution (2.41, 1.77-3.29) and dementia (12.52, 1.86-84.21) were also seen.10 A meta-analysis restricted to surgical patients with hip fracture showed a similar doubling of the hazard ratio of death (2.3, 1.43-3.93; figure ⇓).

Forest plot of data from studies reporting association between delirium after hip fracture and mortality. Meta-analysis done according to published methodology (see Sources and selection criteria).10 Weighting assigned according to inverse of the variance. CI=confidence interval. Mean follow-up period 20 months (range 1-40). Despite significant heterogeneity between the studies (I2=68%) postoperative delirium is associated with increased odds of mortality (defined as >1).
{kind=link}
Despite the association between delirium and postoperative mortality in surgical patients, causality has not been established, and delirium may be just a marker of a complicated postoperative period or reflection of age or comorbidity in this group. None the less, in a cohort study based on retrospective chart review of patients with Alzheimer’s disease, an episode of delirium was associated with a precipitous decline in the patient’s cognitive trajectory.11 Similarly, postoperative delirium has been associated with long term impairments in cognition in prospective cohort studies.12 13 14 Delirium has been studied extensively after critical illness in medical and surgical patients, and is associated with worse clinical outcomes, greater mortality, and prolonged cognitive impairment in survivors.15 Patients who endure emergence or postoperative delirium incur direct morbidity by removing lines and urinary catheters, causing injuries to themselves and to staff.1 Increased costs associated with surgical patients predominantly result from prolonged hospital stay.12 Overall the cost of delirium is estimated to be between $38bn and $152bn per year in the United States (£24-95bn, €27-106bn) .16
Can delirium be prevented in the postoperative period?
Emergence delirium may be prevented by avoiding premedication with benzodiazepines. Prevention of postoperative delirium may be possible through good nursing care with regular patient orientation to time, place, and person, and early mobilisation and rehabilitation.4 Patients who depend on spectacles and hearing aids should be given access to them to reduce the impact of sensory impairment. Irritants such as urinary catheters are best avoided if possible. One randomised controlled trial showed that the involvement of a geriatrician in the perioperative care of patients with hip fracture reduced the risk of delirium by 40%.17 Modifiable risk factors need to be reduced—for example, by ensuring adequate hydration and electrolyte homeostasis, treating pain adequately, and avoiding deliriogenic drugs (such as benzodiazepines or drugs with anticholinergic side effects). The burden of delirium may be reduced by substituting benzodiazepines with another class of sedatives, α2 adrenergic agonists. Two recent trials have shown that patients randomised to the α2 adrenergic agonist dexmedetomidine rather than the benzodiazepines lorazepam18 and midazolam19 were less likely to experience brain dysfunction including delirium. Although meta-analyses of randomised controlled trials have not shown a benefit of regional anaesthesia over general anaesthesia20 for postoperative delirium, a recent randomised controlled trial suggested that light rather than deep sedation with propofol during spinal anaesthesia for hip fracture repair reduced the prevalence of delirium.21 We suggest that limiting the use of GABAergic sedatives (such as benzodiazepines and propofol) could reduce postoperative delirium.6 18 21 Complementing this conclusion, randomised controlled trials have shown that addition of ketamine22 or dexmedetomidine23 to the anaesthetic regimen can reduce the incidence of postoperative delirium. While pain is a common precipitant of postoperative delirium and treatment with morphine has been shown to decrease delirium after hip surgery, opioids may also contribute to the development of delirium if given either in inadequate amounts to control pain or in excess to analgesic needs;24 give opioids judiciously.
Limited evidence supports the use of antipsychotic drugs in the treatment of delirium and the dopaminergic antagonist haloperidol is currently the recommended agent. A randomised controlled trial of haloperidol prophylaxis for hip fracture surgery did not show a reduction in the primary endpoint of the incidence of delirium, but did show reduced severity and duration of delirium (5.4 versus 11.8 days) and reduced length of hospital stay.25 A study using risperidone in patients undergoing cardiac surgery showed a decrease in the incidence of delirium,26 while pilot intensive care studies using haloperidol, ziprasidone, and quetiapine have shown conflicting results compared with placebo.27 28
How should postoperative delirium be managed?
Patients need to be monitored twice daily with use of validated approaches such as the confusion assessment method to detect delirium. For trained staff, the confusion assessment method typically takes about 10 minutes to perform. Experts recommend maintaining patients with delirium in a stable environment with familiar caregivers and providing reassurance.29 Gentle restraint may be necessary to prevent the patient from harm. Identifying and treating any modifiable underlying cause, such as pain, hypoxia, electrolyte abnormalities, or postoperative infection remain the mainstay of treatment.29 Deliriogenic drugs should be discontinued if possible and substituted with alternatives if indicated. At present there is little evidence to support drug treatment, which we suggest should be used only in extreme cases where a patient or their caregivers become at risk, in which case 0.5 to 5.0 mg of haloperidol may be given.25 Further randomised controlled trials are needed to strengthen the evidence base for drug treatment. The α2 agonist dexmedetomidine has shown some promise in critical care delirium, while also reducing duration of mechanical ventilation and duration of intensive care.30
Unlike the improvements in the follow-up of patients with critical care delirium, at present there is little in the way of structured follow-up for all patients who experience postoperative delirium. However, increasing understanding of the long term consequence of the condition indicates that these patients require specialist follow-up.
Is postoperative cognitive decline a pervasive disorder?
While observational evidence suggests that postoperative delirium triggers postoperative cognitive decline, authors of a recent systematic review have noted an absence of evidence that postoperative cognitive decline affects all patients.31 Research into the pervasiveness of postoperative cognitive decline has been hampered by a lack of consensus on how to diagnose the condition and questionable usefulness of cognitive tests. Furthermore, few studies have accounted for the cognitive trajectory of patients from preoperative to postoperative period;31 rather, the majority of studies have assumed that patients are not already experiencing cognitive decline preoperatively. In the few studies where patients were randomised between surgical and non-surgical intervention, cognitive decline occurred equally between the groups;31 these data were supported by a recent cohort study.32 Therefore, although postoperative delirium might sometimes precipitate a long term cognitive decline, present evidence does not suggest that postoperative cognitive decline affects all patients.
Does perioperative care contribute to Alzheimer’s disease?
The association between Alzheimer’s disease and anaesthesia reported in cohort studies led to a flurry of animal studies aimed at exploring the biological plausibility of a link.33 Although findings in animal models suggest that surgery and anaesthesia may increase deposition of amyloid β and tau phosphorylation,34 it is not clear how persistent these changes are. Systematic review and expert opinion of the clinical data surrounding the association of Alzheimer’s disease and perioperative care do not support the association.33
Summary points
Emergence delirium occurs in up to 21% of patients after anaesthesia and surgery but does not seem to induce long term sequelae
Postoperative delirium predominantly affects older people and has been associated with long term increases in cognitive decline and mortality
Emergence delirium can be prevented by avoidance of benzodiazepine premedication
Prevention of postoperative delirium may be possible through good nursing care, regular orientation, early mobilisation and rehabilitation, and avoidance of GABAergic drugs
Management of postoperative delirium involves identifying and treating precipitating factors, patient orientation and protection, stopping deliriogenic drugs (such as benzodiazepines), and judicious use of haloperidol or dexmedetomidine
While postoperative delirium has been associated with cognitive decline, there is a lack of evidence to suggest that cognitive decline is pervasive or that anaesthesia and surgery increase the risk of Alzheimer’s disease.
Tips for non-specialists
For emergence delirium, the mainstay of management is calming reassurance and gentle restraint of the patient to prevent them from harm; identifying and treating associated causes, such as pain, are also important
Postoperative delirium is best managed with good nursing care that promotes patient orientation and early mobilisation, and treatment of any precipitating cause. If necessary consider pharmacological intervention with haloperidol or dexmedetomidine after excluding modifiable causes
Older patients may be reassured that cognitive decline attributable to the perioperative period is rare and usually associated with postoperative delirium. It is probably not pervasive or a cause of Alzheimer’s disease; patients with concerns about postoperative delirium or cognitive decline should be encouraged to speak to their anaesthetist before their operation.
Additional educational resources
For patients
Delirium: quick facts (www.mc.vanderbilt.edu/icudelirium/patients.html)—useful information about delirium for patients and families
For healthcare professionals
Published clinical guidelines: delirium (http://guidance.nice.org.uk/CG103)—guidelines from UK National Institute for Health and Clinical Excellence
About delirium (www.mc.vanderbilt.edu/icudelirium/references.html)—web based reference portal
The confusion assessment method training manual and coding guide (www.hospitalelderlifeprogram.org/pdf/TheConfusionAssessmentMethod.pdf)—further information about the confusion assessment method
Notes
Cite this as: BMJ 2011;343:d4331
Footnotes
Competing interests: All authors have completed the ICMJE disclosure form at www.icmje.org/coi_disclosure.pdf (available on request from the corresponding author) and declare: no support from any organisation for the submitted work; RDS has worked as a consultant for Air Liquide, France, and is a member of the Steering Committee of an Air Liquide sponsored clinical trial exploring the utility of xenon anaesthesia to prevent postoperative delirium. PPP has received funding from Hospira, USA, for clinical trials relating to the use of dexmedetomidine as a critical care sedative and honorariums from Hospira, USA, Orion Pharma, Finland, and Glaxo Smith Klein, United Kingdom. MM has received consultancy fees from Air Liquide, France, and Air Products, USA, regarding the clinical development of xenon and from Hospira and Orion regarding the clinical development of dexmedetomidine; no other relationships or activities that could appear to have influenced the submitted work.
Provenance and peer review: Commissioned, externally peer reviewed.